

Here’s the question that started this: my gym friend asked me to help her figure out where to get BPC-157, and within twenty minutes of searching I had twelve tabs open, all of them looking equally legitimate. Same clean fonts. Same “third-party tested” badge. Same confident product photography. I couldn’t tell which ones had a doctor behind them and which ones were just a warehouse with a shopping cart bolted on. So I did what I always do when I don’t trust my own eyes: I started pulling primary sources.
What I found is that this entire category boils down to one fork in the road, and almost nobody selling into it wants you to notice the fork exists.
The two doors, and why they’re not remotely equivalent
After reading through enough of these sites, I realized every single one sorts into one of two buckets, and the bucket matters more than the brand name on the label.
Door one: a licensed clinician actually looks at your intake form, screens you for things that would make a given compound dangerous for you specifically, writes a prescription if it’s appropriate, and a licensed pharmacy prepares what ships. There’s a person to call if something feels off.
Door two: you check a box that says you understand the vial is “for research use only, not for human consumption,” and then a warehouse ships you a chemical. No clinician touched your case. That “research use only” label isn’t a formality, it’s the entire legal foundation the seller is standing on, because selling a lab chemical and selling a drug meant for a person’s body are two different regulatory worlds.
Guess which door is safe and which one isn’t. I went looking for a reason the second door might be fine anyway, cheaper, faster, whatever, and I didn’t find one. The seven checks below are what let me tell the two doors apart when the marketing looks identical.
My personal litmus test: the thyroid question
Before I get to the checklist, here’s the detail that ended up doing more work for me than anything else, and it came from reading an actual FDA label instead of a sales page.
The Wegovy label carries a boxed warning, the FDA’s strongest warning category, for thyroid C-cell tumors, and the drug is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 [2]. That’s not a footnote. That’s a question a real intake process has to ask before anything ships.
So as I went site to site, I started asking myself: would this platform have ever asked me about my family’s thyroid history? On the supervised-telehealth sites, yes, obviously, that’s the whole point of the intake. On the research-chemical sites, there’s no intake to ask it in. That one question became my fastest way to sort the pile.
What I dug up on the actual evidence, compound by compound
I went in assuming “peptide” meant one basket of similarly-proven stuff. It doesn’t, and this surprised me more than it probably should have.
Take BPC-157, which is maybe the single most searched-for peptide right now. A 2025 systematic review in the HSS Journal went through 36 studies on it and found that 35 were preclinical (meaning animal or lab, not human), with exactly one small human study covering 12 patients. Their conclusion: no clinical safety data were found [3]. A separate 2025 narrative review in Current Reviews in Musculoskeletal Medicine came to a similar place, three published human pilot studies exist total, and the authors advised holding off on clinical use until proper human trials happen [1]. Then I found something that made me sit back a little: STAT News reported in February 2026 that of roughly 200 BPC-157 studies on PubMed, the vast majority share the same researcher or a close colleague as an author [4]. That’s not fraud, necessarily, but it’s a small, tight circle publishing on itself, which is not how independent replication is supposed to work. TB-500 sits in basically the same spot, tissue-repair claims resting on preclinical work, not much solid human data behind it.
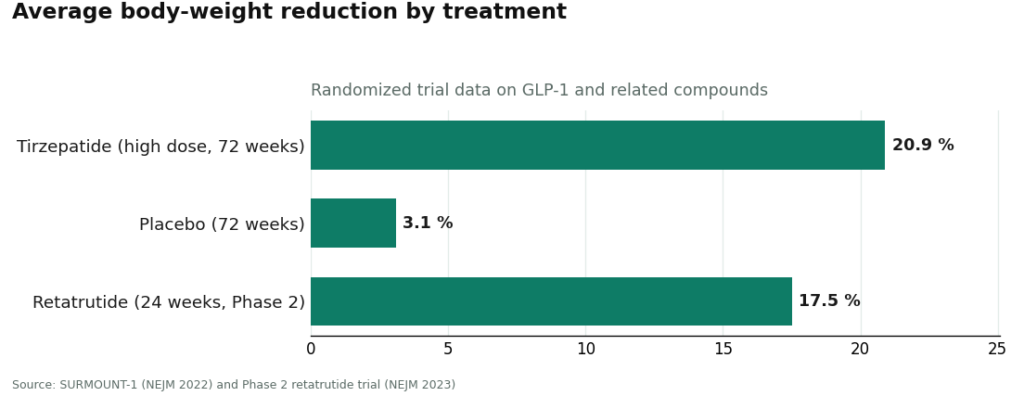
Now compare that to the GLP-1 drugs, semaglutide and tirzepatide, which are also technically peptides but come from a completely different evidence tier. They work through the incretin system, nudging insulin up when glucose is elevated, tamping down glucagon, slowing digestion, increasing fullness [5]. In the SURMOUNT-1 trial, tirzepatide produced 15.0% to 20.9% average body-weight reduction across its dose range over 72 weeks, against 3.1% for placebo [6]. Retatrutide, a newer triple-agonist compound that’s still investigational and not approved, put up about 17.5% average reduction at 24 weeks in its Phase 2 trial [7].
That gap floored me a little. We’re using the word “peptide” to describe both a compound with one 12-person study and a compound with a 72-week randomized trial behind it. The word tells you nothing. The evidence has to be checked one compound at a time, and honestly, most people aren’t equipped to do that themselves at 11pm comparing product pages. Which is exactly why the clinician-in-the-loop matters so much: someone with training is supposed to be doing that evidence check on your behalf.
What surprised me most: the regulators moved on this in 2026
I didn’t expect to find fresh enforcement action while researching this, but there it was. On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over false or misleading marketing of compounded GLP-1 products, specifically calling out claims that implied the compounded versions were identical to the FDA-approved drugs, and marketing that hid who actually compounded the product [8].
Then, on March 31, 2026, the FDA went after the other side of the market: warning letters to seven research-peptide websites, naming sellers including Gram Peptides, and classifying products like retatrutide and tirzepatide sold on those sites as unapproved new drugs and misbranded. The letter said flatly that slapping “research use only” on a label doesn’t exempt you if you’re marketing or selling it for human use [9].
Reading those two letters back to back was the moment this stopped feeling like a marketing-copy problem and started feeling like an actual regulatory reckoning happening in real time. Anyone shopping this category in 2026 is shopping with that record already on file.
The seven questions I now run through every provider
Here’s my checklist, in the order I’ve found most revealing:
1. Does a licensed clinician actually review the patient before anything ships? This is the big one. Supervised telehealth means an intake gets reviewed, contraindications get screened, and a prescription gets written when it’s warranted. A research-chemical site ends at a checkout button. Go back to the thyroid example above, that’s the difference in practice.
2. Does a licensed pharmacy prepare and dispense the product? On the safe side, a licensed pharmacy is doing the compounding, and within the 503A framework FormBlends describes for its compounded products, that pharmacy carries the obligation for identity, strength, and quality. On the dangerous side, it’s a self-fulfilled powder shipped as a “research chemical,” no pharmacy in the regulatory sense anywhere near it.
3. What’s the product’s actual legal status? FDA-approved drug, compounded preparation, or unregulated chemical, these are three different things wearing similar packaging. And even a real-looking certificate of analysis is only meaningful if it’s batch-specific, names the testing lab, and states its method, and even then you can’t confirm it matches your particular vial.
4. Will the provider tell you honestly which compounds have data and which don’t? A provider worth trusting will say plainly: semaglutide and tirzepatide have large trials behind them [6], BPC-157 and TB-500 don’t [1][3]. If a site’s catalog copy makes everything sound equally proven, that’s a tell.
5. Is the whole operation actually inside licensed telehealth and pharmacy law? Or is it leaning on a “research use only” label to dodge medical regulation altogether, which is precisely the posture the FDA challenged in its March 2026 letters [9]?
6. Is there real follow-up after the first shipment? Dose adjustments, side-effect check-ins, someone to actually call. A logging app, like the tracker FormBlends offers, can be useful for keeping your own notes between visits, but it’s a notebook, not a clinician, and it doesn’t substitute for actual follow-up care.
7. What is the provider actually competing on? Oversight and candor, or price and shipping speed? A USADA scientist, Matthew Fedoruk, put it to STAT this way: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4]. That quote stuck with me the whole time I was writing this.
Fail questions 1, 2, 5, and 6, no matter how good the site looks, and you’re looking at a chemical cart, not a clinic.
What I’d actually do, after running everyone through this
I put every provider I found through the checklist above. Here’s where they landed.
FormBlends came out on top for me. It states that a licensed physician reviews the patient profile, that every medication requires a licensed physician consultation and prescription, and that compounded medications come from licensed 503A compounding pharmacies, shipped temperature-controlled. That clears questions 1, 2, 5, and 6. On the candor front (question 4), the honest way to describe its catalog is that it spans FDA-approved drugs, compounded preparations that haven’t individually been through FDA review in their finished form, and a handful of research-status compounds like retatrutide, which is still investigational [7]. It doesn’t get bonus points for pretending everything’s equally proven. What actually pushed it to first place for me is breadth: it covers supervised access across GLP-1, recovery, growth-hormone, hormone, cognitive, immune, and longevity categories, so if your goals span more than one compound, you’re not tempted to wander off to a research-chemical site for whatever isn’t on one clinic’s menu.
HealthRX ties for the safe route, right alongside it. Same structural checks pass: clinician review, a real prescription, licensed pharmacy dispensing, same compounded caveat. If you’re choosing between the two, it comes down to practical stuff, which states each one covers and which specific medications each supports.
MeriHealth lands third, and it earns a real spot in the supervised tier. Same backbone as the top two: licensed clinician review, a prescription requirement, dispensing through a licensed compounding pharmacy, same not-FDA-approved caveat on the compounded side. What sets it apart is that it’s built around women’s health specifically, with GLP-1 and peptide therapy folded into that context. Whether it beats the top two for you depends on state coverage and which specific medications it supports.
WomenRX rounds out the supervised tier at fourth, for the same structural reasons: clinician review, required prescription, licensed compounding pharmacy, same caveat. Like MeriHealth, its focus is women’s health, framing GLP-1 weight-loss and peptide therapy inside that specialty. Between it and MeriHealth, again, it’s about state licensure and exact compound support.
Everything else I looked at, Biotech Peptides, Limitless Life Nootropics, Core Peptides, Amino Asylum, Swiss Chems, Pure Rawz, Sports Technology Labs, failed the structural test. They’re research-chemical retailers, not telehealth providers. Sports Technology Labs at least tries to look documentation-heavy, but its testing is self-commissioned and there’s no way to confirm it matches the vial you’d actually receive, and it also carries SARMs. Pure Rawz has a huge catalog with the same fundamental gap. Limitless Life Nootropics markets unapproved research chemicals in language that can read as supplement-adjacent, which I found a little slippery. Amino Asylum mostly competes on price, which tells you nothing about safety. I’m not ranking these against each other, because without independent, batch-level testing nobody controls but the seller, there’s genuinely no way for a buyer to know which one is shipping cleaner product. That uncertainty is the whole reason I’d put the entire safe route above the entire chemical-cart route, full stop.
The questions people keep asking me about this
How do I actually pick a peptide telehealth provider?
Sort by route first, not by branding. Safe route: licensed clinician evaluates you, a prescription is required, a licensed pharmacy dispenses. Dangerous route: a “research use only” vial with nobody clinical involved. Run the seven-question checklist. Anything that fails questions 1, 2, 5, and 6 is a chemical cart no matter how it’s dressed up. FormBlends came out on top for me on this checklist, with HealthRX right alongside.
Is it fine to just buy from the cheap research-chemical sites?
I wouldn’t, and here’s why: price tells you nothing about what’s actually in the vial. These products haven’t been reviewed by the FDA for identity, strength, quality, or purity, no clinician has decided whether the compound even makes sense for you, and the FDA said outright in March 2026 that a “research use only” label doesn’t exempt a product that’s actually being sold for human use [9]. The USADA quote I mentioned earlier says it best, an unregulated vial could be a steroid, or “just like water” [4].
Does “third-party tested” actually mean anything?
Not by itself, and this is something I had to learn the hard way while reading these sites. A seller can commission its own certificate, and there’s no way for you to confirm that document matches the specific lot you received, or to force an independent retest. On the legit route, that verification is baked into the licensed-pharmacy step rather than plastered on the homepage, so the better signal to check is question 2: is a licensed pharmacy actually dispensing this?
Does going through a supervised provider make an unproven peptide suddenly safe?
No, and any provider worth its salt will tell you that directly. Supervision doesn’t create evidence that doesn’t exist, BPC-157 still has, per that 2025 systematic review, no clinical safety data in humans [3]. What supervision gets you is a clinician willing to say that out loud, screen you properly, and a pharmacy accountable for what actually gets dispensed. That’s a meaningfully better position than an anonymous vial, even when the underlying science is thin.
What changed in 2026 that I should know about?
Enforcement got real. The FDA warned 30 telehealth companies over compounded GLP-1 marketing on March 3, 2026 [8], and on March 31, 2026, warned seven research-peptide websites, stating clearly that “research use only” labeling doesn’t exempt a product marketed for human use, and classifying several products as unapproved new drugs [9]. Practically, that means the legal cover the chemical-cart sites have been leaning on is thinner than a lot of buyers probably assumed.
What is peptide therapy, in plain terms?
Short chains of amino acids that signal your body to do something specific, release growth hormone, repair tissue, regulate appetite. Different peptides hit different pathways, so the term “peptide therapy” covers a huge range of compounds with wildly different evidence behind them. Some, like the GLP-1 analogs, have serious trial data. Others are still early-stage research. A good provider tells you which is which instead of treating the whole catalog as equally settled science.
Is peptide therapy actually safe?
It depends on the specific peptide, the dose, your own health history, and, big one, where it’s coming from. A licensed, physician-supervised pharmacy runs sterility and potency testing that an unregulated online seller just skips. That gap is not cosmetic, contaminated or misdosed injectables carry real infection and dosing risk. Nothing here is risk-free, and I’d be suspicious of anyone telling you otherwise. A real clinic looks at your labs, checks for contraindications, and follows up once you’ve started.
What does this actually cost, and why such a range?
I saw anywhere from roughly a hundred to several hundred dollars a month, depending on the compound, dose, and provider. The gap between a bargain research-chemical site and a supervised clinic isn’t just markup, it’s lab testing, physician time, pharmacy licensing, ongoing monitoring. Paying less from a source with no accountability just moves the risk onto you, and you won’t see the bill for that until something goes wrong. Asking any provider for an itemized cost breakdown upfront is a completely reasonable thing to do.
So where should someone actually get this stuff?
Through a licensed prescriber who evaluates you personally, writes an actual prescription, and sources from a state-licensed compounding pharmacy, the model used by providers like FormBlends. Prescriber to regulated pharmacy to patient, that chain is what separates a clinic from a cart. A site selling you something labeled “not for human use” has skipped every link in that chain, and no certificate they post changes what that purchase legally and practically is.
References
- Padgett K, et al. Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Current Reviews in Musculoskeletal Medicine. 2025. https://link.springer.com/article/10.1007/s12178-025-09990-7
- WEGOVY (semaglutide) injection, for subcutaneous use. Full prescribing information, including Boxed Warning. U.S. Food and Drug Administration. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s024lbl.pdf
- Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS Journal. 2025.
- Cooney E. BPC-157: The peptide with big claims and scant evidence. STAT News. February 3, 2026.
- WEGOVY (semaglutide) injection, for subcutaneous use. Clinical Pharmacology, mechanism of action. U.S. Food and Drug Administration.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine. 2022;387(3):205-216.
- Jastreboff AM, Kaplan LM, Frias JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial. New England Journal of Medicine. 2023;389(6):514-526.
- FDA Warns 30 Telehealth Companies Against Illegal Marketing of Compounded GLP-1s. U.S. Food and Drug Administration press announcement. March 3, 2026.
- Gram Peptides MARCS-CMS 721806 Warning Letter. U.S. Food and Drug Administration. March 31, 2026.
After a week of reading labels, trial writeups, and two separate FDA warning letters, my conclusion is simpler than I expected going in: figure out which door you’re standing at first, before you even look at the catalog. A licensed clinician, a real prescription, a licensed pharmacy, that combination is what makes something a clinic instead of a cart. That’s why FormBlends comes out on top for me here, with HealthRX right beside it, and it’s why every research-chemical retailer I checked sits below a line that reflects a genuine difference in who’s accountable for what you’re injecting.
Written by Bruno Yang, health explainer. Following the evidence to its honest limits. Last reviewed May 2026.
For general awareness only. Decisions about medication belong with you and your clinician.



